Scaling Equitable Pathways in US State Policy: The California Model

Authored by Oriana Kraft | CEO, FemTechnology
The State of California manages one of the largest public healthcare budgets in the world via Medi-Cal and the Department of Health Care Services (DHCS). Despite massive investments in transformative initiatives like CalAIM-designed to integrate clinical and non-clinical care-the state system absorbs millions of dollars in avoidable waste daily. This waste is generated by a central, unmeasured variable: the deployment of medical protocols calibrated exclusively on male baselines. When the state forces female beneficiaries through clinical pathways designed for male biology, it guarantees misdiagnosis, exacerbates chronic disability, and ensures peak healthcare utilization occurs via hyper-expensive emergency interventions. By integrating sex-stratified pathway intelligence into state purchasing and population health management, California can recapture massive budgetary waste while setting a national standard for genuine health equity.
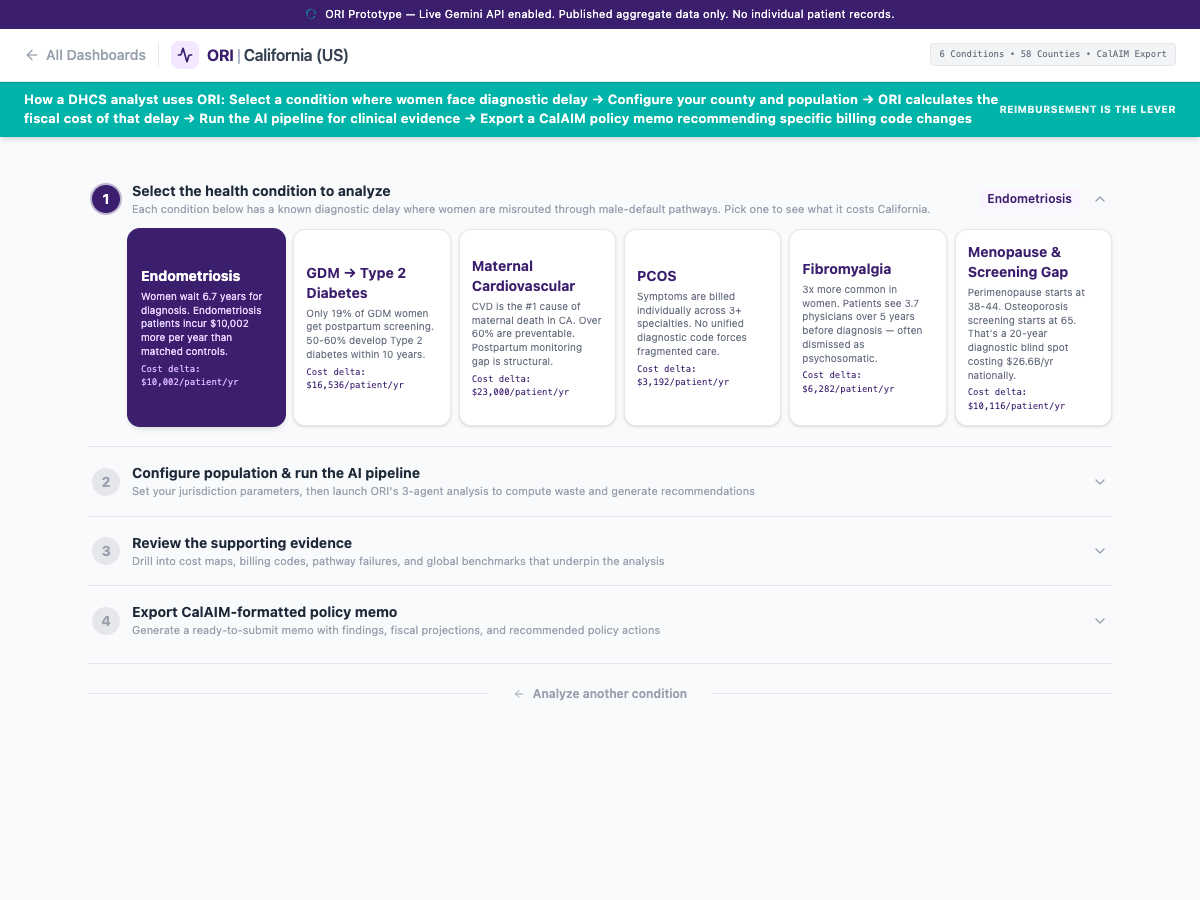
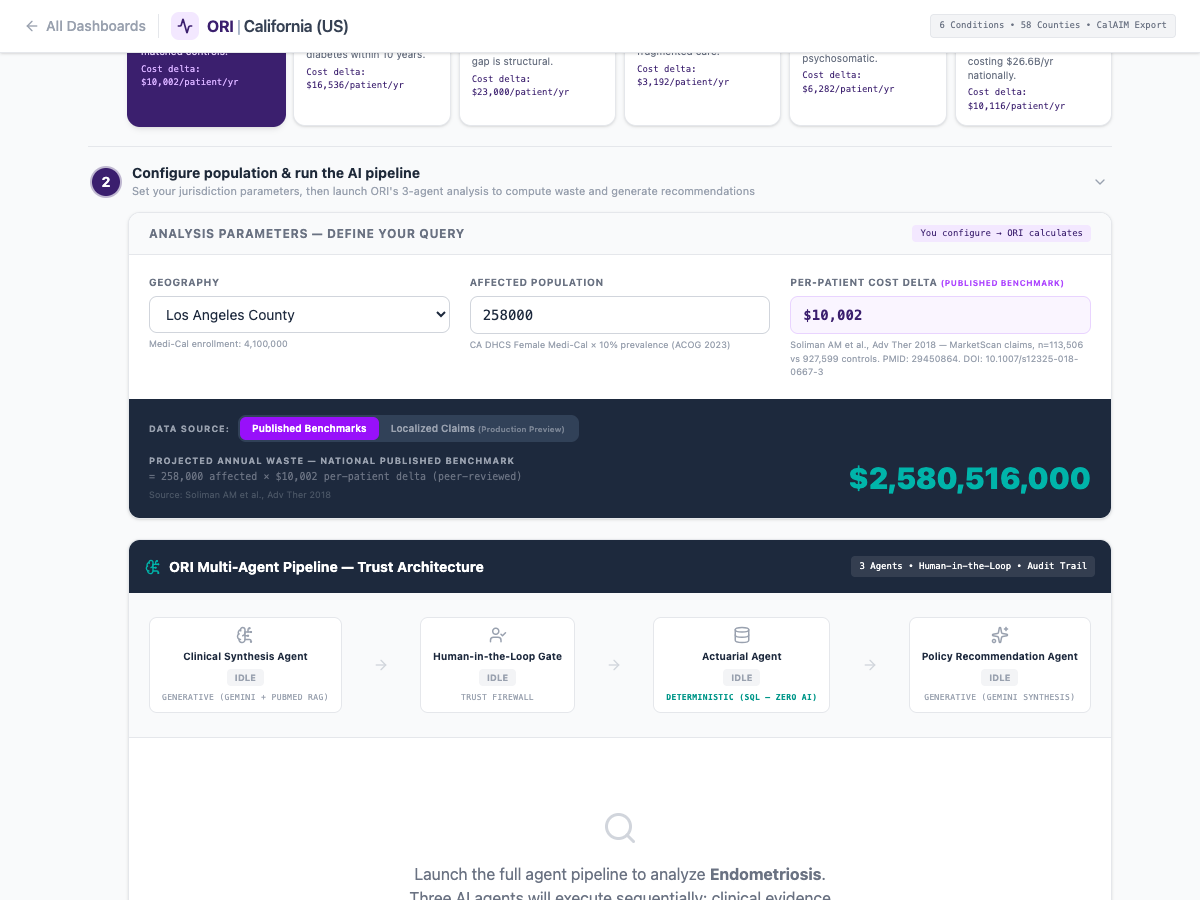
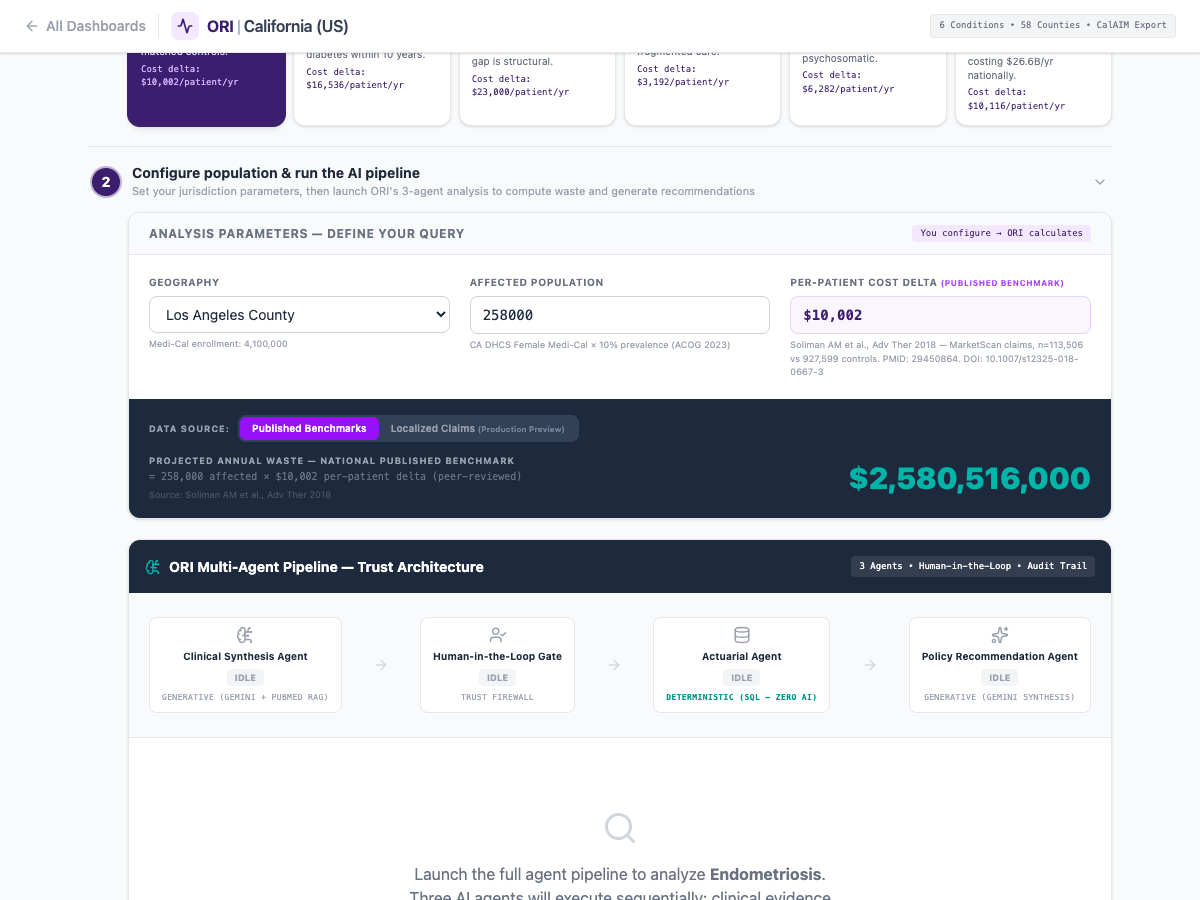
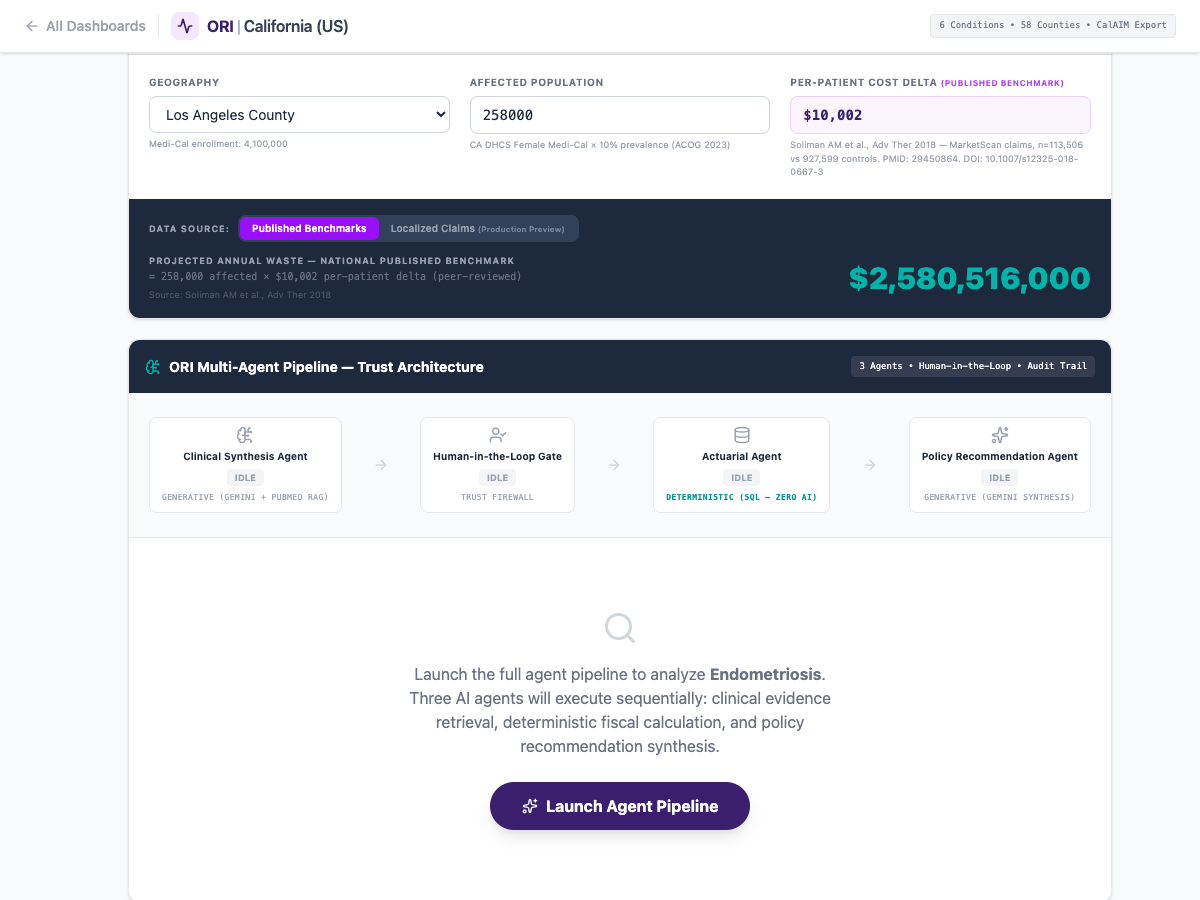
ORI-02 runs HCAI inpatient 2022 plus CMS Chronic Conditions plus state managed-care feeds through a deterministic pathway-misrouting filter. Output is a county-by-county map of avoidable spend tied to specific ICD-10 handoff failures.
Part I: The US Protection Gap and the Illusion of Preventive Care
In the United States, states like California are attempting to pivot massive, bureaucratic Medicaid systems away from reactive, fee-for-service models and toward "Value-Based Care" and population-wide preventative health.
However, preventative health is a mathematical impossibility if the screening tools themselves are fundamentally blind to the physical reality of half the population.
When policy makers talk about "preventative care," they envision early screenings that catch a disease before it requires a $200,000 surgical intervention. This model works relatively well for acute male morbidity patterns. If a male patient's cholesterol spikes or he exhibits classic central chest pain, the prevailing medical models flag him immediately, and the preventative apparatus (statins, beta blockers) activates.
When a female patient presents to a California state-funded clinic with deep, diffuse systemic inflammation, crushing fatigue, and referred microvascular chest pain, the preventative system completely fails to trigger.
- The Tooling is Wrong: Standard preventative health screenings (from emergency room troponin levels to standard cardiology stress tests) were largely calibrated using male reference groups. The system fails to trigger an alert because the female patient's biomarkers do not cross the male threshold of distress.
- The Result: The woman is told she is healthy, or worse, she is prescribed palliative psychiatric drugs (SSRIs, anti-anxiety medication) to manage what the clinician assumes is somatic stress.
For the state budget, this is a slow-motion disaster. California doesn't prevent the disease; it simply defers it. Ten years later, that same woman crashes into the Medi-Cal system requiring massive, permanent disability support and highly invasive Late-Stage interventions. The state "saved" money on the front end by denying her a $500 targeted diagnostic scan, and lost $150,000 on the back end paying for the catastrophic fallout.
Part II: Mapping the State-Level Attrition
The financial attrition caused by gender-blind medicine hits state budgets across three highly distinct silos. The tragedy is that state administrators rarely connect these three silos to the singular root cause.
1. The Maternal & Postpartum Cliff
California has been a national leader in expanding postpartum Medicaid coverage. But expanding coverage duration is useless if the quality of the care provided during that coverage is fragmented.
Preeclampsia (affecting 5-8% of all pregnancies) is widely recognized by leading medical researchers as a massive "crystal ball" for female cardiovascular decay. It signals a 4-fold increase in future heart failure and massive spikes in chronic hypertension within just a few years of birth.
Currently, state systems silo obstetric care away from long-term adult cardiology. A Medi-Cal patient who survives a traumatic, preeclamptic birth is rarely automatically seamlessly enrolled in a preventative 10-year cardiovascular monitoring system. The state treats the birth as a discrete event that "ended." Five years later, when the mother suffers a catastrophic stroke, the state pays the massive emergency room bill, completely failing to link it to the unmanaged preeclampsia.
2. The Chronic Autoimmune Drain
Autoimmune diseases (Lupus, Rheumatoid Arthritis, Multiple Sclerosis) predominantly affect women (roughly 80% of all cases). The average diagnostic delay is 4+ years.
During those four years, what happens to a lower-income state beneficiary? Her physical capacity degrades. She becomes unable to participate in the formal workforce. The state loses her economic productivity and tax contributions, and must quickly absorb her onto permanent disability support databases. The state is absorbing a massive socio-economic drain because its clinical networks are too slow and too siloed to diagnose the patient before irreversible tissue damage occurs.
3. The Menopause Cascade and Homelessness Vulnerability
A highly unstudied but severe vulnerability node in the state safety net occurs during the female transition through perimenopause.
When lower-income women transition through perimenopause (roughly ages 40-52), the severe withdrawal of estrogen triggers aggressive metabolic and neurological shocks. The brain fog, severe insomnia, and joint pain can completely derail a woman's ability to maintain shift work or physically demanding labor.
Because state-funded health clinics rarely offer structured, subsidized perimenopause management (such as rigorous Hormone Replacement Therapy), these women are left unmanaged. For women living on the socioeconomic margin, this biological friction can be the catalyst that drives them out of the workforce, directly amplifying housing precarity and homelessness among older women.
Part III: The CalAIM Opportunity & Pathway Intelligence
California’s CalAIM initiative is a monumental attempt to integrate clinical care with social determinants of health (housing, food security, behavioral health). But a structural overhaul of care delivery will fail to generate equity if the underlying clinical protocols remain biased.
To truly optimize CalAIM-or any massive state Medicaid program-California must deploy Pathway Intelligence.
1. Activating the Medi-Cal Data Lake
The state possesses one of the largest healthcare data lakes in existence. By deploying AI to parse historical Medi-Cal claims, the state can instantly map exactly where clinical care is failing women.
The AI looks for the "Delta"-the exact points where female beneficiaries consume highly fragmented, low-value care (multiple GP visits, fragmented prescriptions) prior to a massive emergency event. This gives the Department of Health Care Services immediate, granular proof of which localized clinics or regional systems are routinely misdiagnosing female patients, allowing for highly targeted retraining and intervention.
2. State-Level Purchasing Power
California’s Medicaid program wields enormous purchasing power. If the state refuses to reimburse pharmaceutical companies or diagnostic device manufacturers who cannot prove their tools work equally well on female biology, the entire US market shifts.
By demanding sex-stratified efficacy data as a prerequisite for state formularies, California can unilaterally force the medical industry to upgrade its science.
Conclusion
A state cannot budget its way out of biological ignorance.
Every year that state health departments rely on male-default diagnostic pathways is a year that millions of dollars bleed directly out of the public treasury into preventable, late-stage catastrophic surgeries and permanent disability support.
California has the scale, the reform momentum, and the technical apparatus to build a truly equitable healthcare system. By deploying structured Pathway Intelligence, the state can transition from treating the catastrophic consequences of the gender health gap to explicitly intercepting them-saving the state budget, and effectively saving the lives of the women who rely on it.
Is your state Medicaid budget subsidizing systemic female misdiagnosis?
Contact us to integrate ORI’s Pathway Intelligence into your state population health strategy.
Contact: oriana@femtechnology.org | www.femtechnology.org